Diabetes mellitus and Carbohydrate disorder
Population Doubling Time in
Some Mediterranean Countries
(HYPOGLYCEMIA
(INSULIN REACTIONS
The blood glucose falls to less than
50 -60 mg/dL.
It can be caused by too much insulin
or oral hypoglycemic agents, too
little food, or excessive physical
activity.
It often occurs before meals,
especially if meals are delayed or
snacks are omitted.
The blood glucose falls to less than
50 -60 mg/dL.
It can be caused by too much insulin
or oral hypoglycemic agents, too
little food, or excessive physical
activity.
It often occurs before meals,
especially if meals are delayed or
snacks are omitted.
Clinical Manifestations
The clinical manifestations of hypoglycemia
may be grouped into two categories:
1-adrenergic symptoms
2-central nervous system (CNS) symptoms.
In mild hypoglycemia, as the blood glucose level falls, the sympathetic nervous system is stimulated, resulting in a rise of epinephrine or nor epinephrine.
This causes symptoms such as sweating, tremor, tachycardia, palpitation, nervousness, and hunger
In moderate hypoglycemia, the fall in blood glucose
level
deprives the brain cells of needed fuel for functioning.
Signs of impaired function of the CNS
may include inability to
concentrate, headache, lightheadedness, confusion, memory
lapses, numbness of the lips and tongue, slurred speech, impaired
coordination, emotional changes, irrational or combative
behavior, double vision, and drowsiness.
In severe hypoglycemia, CNS function is
so impaired. Symptoms
may include disoriented behavior, seizures, difficulty arousing
from sleep, or loss of consciousness
Diabetic Ketoacidosis (DKA)
Diabetic ketoacidosis (DKA) is
an acute metabolic complication of diabetes characterized by hyperglycemia,
hyperketonemia, and metabolic acidosis. DKA occurs mostly in type 1 diabetes.
It causes nausea, vomiting, and abdominal pain and can progress to cerebral
edema, coma, and death. DKA is diagnosed by detection of hyperketonemia and
anion gap metabolic acidosis in the presence of hyperglycemia. Treatment
involves volume expansion, insulin replacement, and prevention of hypokalemia.
Nonketotic Hyperosmolar
Syndrome (NKHS)
Nonketotic hyperosmolar
syndrome (NKHS) is a metabolic complication of diabetes mellitus (DM)
characterized by hyperglycemia, extreme dehydration, hyperosmolar plasma, and
altered consciousness. It most often occurs in type 2 DM, often in the setting
of physiologic stress. NKHS is diagnosed by severe hyperglycemia and serum
hyperosmolarity and absence of significant ketosis. Treatment is IV saline
solution and insulin. Complications include coma, seizures, and death
Nutrition and diabetes
Nutritional management of DM should
start with nutritional assessment.
Food for diabetic people should be:
High in starchy carbohydrates
High in NSP (fibre)
Low in salt and sugar (not sugar free)
Low in fat (mainly saturated fat)
Having diabetes doesn't mean that you
have to start eating special foods.
Rather than a restrictive diet, a diabetic
diet is a healthy-eating plan that is
rich in nutrients and doesn’t differ
from diet considered healthy for
everyone.
Establish a routine for eating meals.
Consistency is a key.
Artificial sweetening agent
Sugar substitutes that contain little or
no calories are called artificial
sweeteners, non-nutritive sweeteners or
non-caloric sweeteners.
Well-known artificial sweeteners include
saccharin, sucralose and aspartame.
Nutritive sweeteners include sucrose
and fructose.
Artificial sweetening
agents(cont)
Moderate use of nutritive (sucrose and
fructose) and non-nutritive sweeteners
(saccharin, aspartame and cyclamate)
can be part of a well-balanced diet for
diabetics.
However, diabetic patients, as other
people, should accustom themselves to
the low-sweetness taste.
Diet
Water intake should be decreased
when passing large amounts of urine.
All carbohydrates should be
removed from the diet.
Honey is good for diabetes
control.
Consuming bitter &/or salty foods buffers hyperglycemia.
Treatment
Medications in the form of
insulin or oral agents suppress pancreatic activity and cause habituation.
Medications should be stopped
during acute illness.
Herbal therapy is more
efficacious and safer than insulin or oral agents.
Tablets are oral insulin.
Insulin
Affects the eyes, the liver
and the kidneys adversely.
Addictive (once insulin,
always insulin).
Not to be taken for fear of
hypoglycemia.
Insulin leads to pancreatic
failure.
Carbohydrate metabolism disorder
First we will talk about the
normal Carbohydrate metabolism in the body
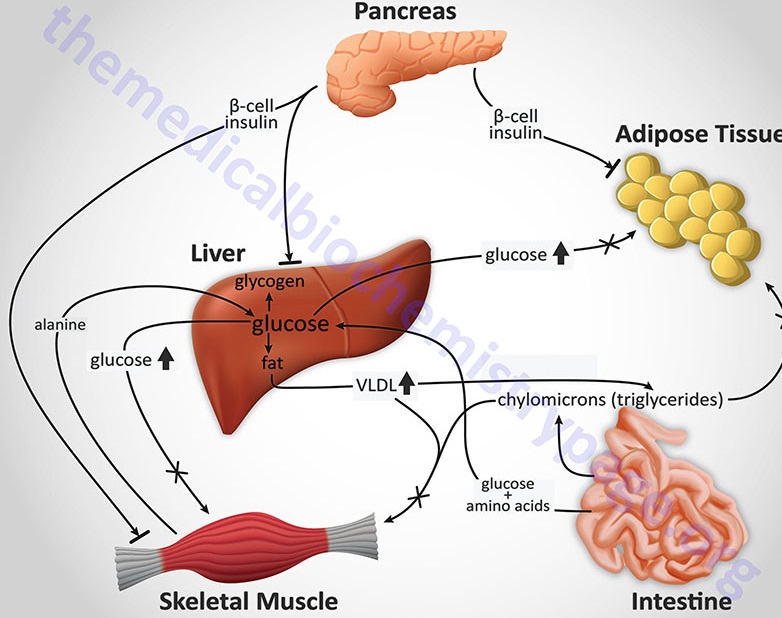
Carbohydrate metabolism begins
with digestion in the small intestine where monosaccharides are absorbed into
the blood stream. Blood sugar concentrations are controlled by three hormones:
insulin, glucagon, and epinephrine. If the concentration of glucose in the
blood is too high, insulin is secreted by the pancreas. Insulin stimulates the
transfer of glucose into the cells, especially in the liver and muscles,
although other organs are also able to metabolize glucose
In the liver and muscles, most
of the glucose is changed into glycogen by the process of glycogenesis
(anabolism). Glycogen is stored in the liver and muscles until needed at some
later time when glucose levels are low. If blood glucose levels are low, then
eqinephrine and glucogon hormones are secreted to stimulate the conversion of
glycogen to glucose. This process is called glycogenolysis (catabolism).
If glucose is needed
immediately upon entering the cells to supply energy, it begins the metabolic
process called glycoysis (catabolism). The end products of glycolysis are
pyruvic acid and ATP
During strenuous muscular
activity, pyruvic acid is converted into lactic acid rather thatn acetyl CoA.
Durlng the resting period, the lactic acid is converted back to pyruvic acid.
The pyruvic acid in turn is converted back to glucose by the process called
gluconeogenesis (anabolism). If the glucose is not needed at that moment, it is
converted into glycogen by glycogenesis
Carbohydrate Metabolism
Disorders
The metabolism of the
carbohydrates galactose, fructose, and glucose is intricately
linked through interactions between different enzymatic pathways, and disorders
that affect these pathways may have symptoms ranging from mild to severe or
even life-threatening. Clinical features include various combinations of hypoglycemia
(low blood sugar), liver enlargement, and muscle pain.
Glycogen Storage Diseases 1-
Glycogen storage diseases are
caused by deficiencies of enzymes involved in glycogen synthesis or breakdown;
the deficiencies may occur in the liver or muscles and cause hypoglycemia or
deposition of abnormal amounts or types of glycogen (or its intermediate
metabolites) in tissues
Defects in glycolysis (rare) may cause syndromes similar to GSDs.
2-Galactosemia
Galactosemia is caused by
inherited deficiencies in enzymes that convert galactose to glucose. Symptoms
and signs include hepatic and renal dysfunction, cognitive deficits, cataracts,
and premature ovarian failure. Diagnosis is by enzyme analysis of RBCs.
Treatment is dietary elimination of galactose.
Galactose is found in dairy
products, fruits, and vegetables .
3-Disorders of Fructose
Metabolism
Deficiency of enzymes that
metabolize fructose may be asymptomatic or cause hypoglycemia, nausea and vomiting,
abdominal pain, sweating, tremors, confusion, lethargy, seizures, and coma.
Fructose is a monosaccharide
that is present in high concentrations in fruit and honey and is a constituent
of sucrose and sorbitol.
4-Disorders of Pyruvate
Metabolism
Inability to metabolize
pyruvate causes lactic acidosis and a variety of CNS abnormalities.
Pyruvate is an important
substrate in carbohydrate metabolism
Pyruvate dehydrogenase deficiency: Pyruvate dehydrogenase is a multi-enzyme complex responsible for the generation of acetyl CoA from pyruvate for the Krebs cycle. Deficiency results in elevation of pyruvate and thus elevation of lactic acid levels
OTHER DISORDERS OF
CARBOHYDRATE METABOLISM
Phosphoenolpyruvate
carboxykinase deficiency impairs gluconeogenesis and
results in symptoms and signs similar to the hepatic forms of glycogen storage
disease but without hepatic glycogen accumulation .
References:
http://www.merck.com/mmpe/sec12/ch158/ch158d.html
http://www.mendosa.com/gilists.htm
http://www.elmhurst.edu/~chm/vchembook/600glycolysis.html
No comments:
Post a Comment